
Crash courses and Workflow of PGY1 Medicine
Working Night Shift
- Find out who you are working with: Legacyhealth.sharepoint.com - legacy salmon creek
https://oncall.lhs.org/smartweb/pages/oncall/oncall_search.jsf
- Sign on to the inpatient team: Log in Epic, LSC resident A or B,
- Sign In and write your number to assign 10/12 hours shift.
- Read through each patient handoff and write to do lists with alarm.
Admissions Checklist for the Nights
- If possible, be with the attending to call the EM doctor to gather information.
- If not, Go view the ED summary (pre-charting)
- Admissions tab & Order set & start there.
1. Medicine Reconciliation/ Allergies (sure script / pcp note / pharmacy consult if pt not coherent)
2. Problem list formulation as you populate note and chart
3. See patient physical exam ROS = meds / allergy / code status/ pmh / bleeding clotting/ DM HTN / Pain / Chronic condition heart / COPD / surgical history / drug alcohol use
4. Intervention / brain storming comes after
Bowel Regimen
Start Bowel regimen in all hospital patients as the inpatient setting is prone to constipation.
-
Osmotic (PEG) polyethylene glycol "Miralax" 17 g qAM
-
Stimulant Senna 17.2 g qHS ..SD
-
If this doesnt work, consider upgrading stimulant Senna to Bisacodyl.
-
Mg class are great (Milk of Mg 30-60mL) vs (Mg Citrate 300 mL)
-
Still constipated: consider lactulose 30 mg q2hr until poop or suppository bisacodyl
-
Golytely bowel prep drink: effective but too much volume
-
-
Opioid induced constipation
1. reduce the opioid dose if possible
2. Oral Naloxone 4 mg dissolved in water cup (3% bioavailability via oral formulation = more gut)
3. Methylnaltrexone
Docusate usages are falling out of favor: 2014 Nov Can Journal of Gastro /Hepatology

Pain Regimen
Tylenol: 650 mg every 4 hours /PRN vs 1000 mg every 6 hours /PRN
• Daily maximum of 4 gram for patients with healthy liver. 2 g for compromised liver
• Toxicity around 10 gram
• schedule the dose q4h or q6h because if it is in PRN, they will be missing out.
• oral / rectal tablet
• IV expensive
NSAIDS: avoid in GI bleed, AKI, CKD (older pts) ; 400 mg PO every 6 hours or PRN
• Motrin/Advil 400 mg PO q 6 - 8 hours
• Aleve Naproxen: q12h
• Ketorolac / Toradol (IV useful for those who cannot tolerate oral): useful in Kidney Stone
• Indomethacin 50 mg TID during gout (generally 20 mg TID for other pain)
Lidocaine Patch 5% 700 mg 24hour application
• Maximum of 3 patch per day.
• Place for 24 hours and remove.
Capsaicin Cream
Burning sensation that leads to numbess via binding to nocioceptors and reducing sensitivity/desensitization.
• Most effective OA (0.025% Cream)
• Neuropathic pain (0.075% cream)
Double-blind trial showing 80% of patients with osteoarthritis had reduced pain after 2 weeks: https://pubmed.ncbi.nlm.nih.gov/1954640/
Diclofenac (Voltaren) Gel apply 4 x daily
• 1% for OA
• 3 % for actinic keratosis
• low risk of systemic absorption
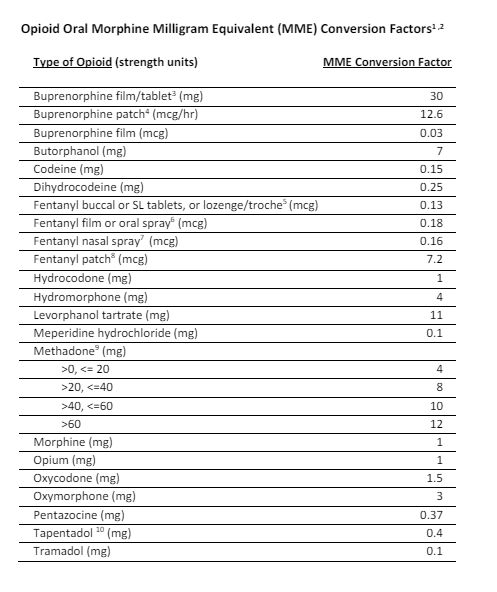
Opioids/ add naloxone on order
Tramadol (partial mu/5HT) agonist
• lowers seizure threshould, different response rate
• Dose 50 mg q 4 hours or as needed
Oxycodone
• Dose 5 mg (50% dose if small, child, elderly) ; onset 30 min ; lasts 3- 6 hours
Oxycontin lasts 12 hours ER
Dilaudid/Hydromorphone
• Rapid onset = euphoria
• Liver metabolized (avoid)
Morphine
• hospice, air hunger
• MS CONTIN (ER) / Roxonol (Liquid)
• Metabolized by Kidney (avoid CKD)
Outpatient meds (OPIOID)
• Norco: hydrocodone/acetomenophen
• Vicodine/Percocet: Oxycodone/acetomenophen
ED/Acute herniated Disc: Back sprain cocktail as per Dr. Qanda
-
Methylprednisolone 2mg
-
NSAID/Tylenol (400 - 650mg)
-
Valium 2mg for muscle relaxant.
-
Opioid + BZO is never a safe thing, if you must use it do it safely = lowest dose.
Misc
UroJet - Lidocaine gel for painful foley.
Neuropathic pain: Gabapentin, Cymbalta, Effexor, TCA
Methadone= long acting trying to wean off opioid (IV cause QT prolongation while PO does not)
Ketamine = Dose: 0.1-0.35 mg/kg/dose IV x1; Alt: 0.1-1 mg/kg/h IV prn; Info: refer to institution protocols
Buprenorphine = partial agonist with low resp depression. Dosing uncertain for pain with sublingual.

Electrolyte Replacement Guide
Vanderbilt Electrolyte Replacement protocol. hyperlink
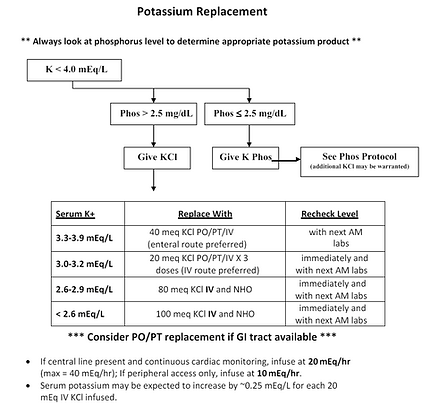
Potassium Replacement problematic <3.5 or >4.5
• Usually 10 mEq = 0.1 increase
• Severely hypokalemia ie 3.0, will require more than 10 mEq to raise 0.1.
• AKI / CKD if you must replace, give 50% of dose reduction.
• KCL SR table (big) / KCL oral liquid / KCL IV (burns and 10mEq is 50 mL of volume for HF patients)
• IV peripheral rate: 10 mEq/hr
• IV central excess: 20 mEq/hr
Question: How quickly can you correct potassium if they are 3.0 mEq/L and require PO/ IV/ PT x 3 ?
Notify Hosptial Officer**
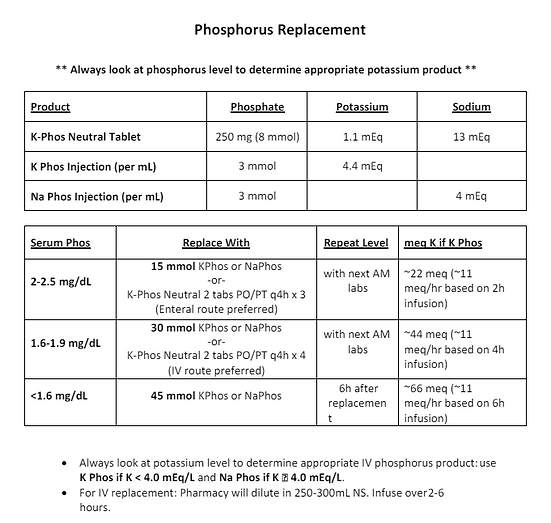
Magnesium: blocks the distal collecting tubule potassium efflux channel. Without it, potassium cannot be corrected.
• 1 gram IV magnesium sulfate will increase 0.1 serum level **** Choose this
• 400 mg PO magnesium oxide tablet is equivalent to 2 gram IV **** Diarrhea
hypomagnesium can cause hypocalcemia due to resistence to PTH
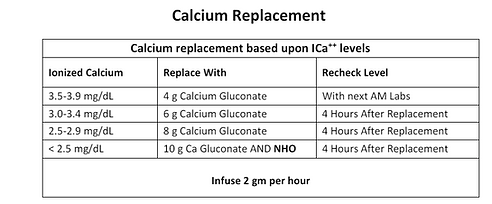
Calcium / use albumin correction as ions bind to albumin
• Corrected Ca = (4 - Albumin) x 0.8 + Ca (serum ionized Ca just tells you correction directly tho)
• Choices include: Calcium chloride IV, Calcium gluconate IV, Calcium Carbonate Tums, Calcium Citrate
Calcium less than 7.5 or ionized serum less than 0.8 gets IV all else to PO.
Refractory hypocalcemia can be due to magnesium low / CKD (PTH)
Effects of low calcium = perioral numbness -> Trousseau's sign (involuntary contraction of arm hand) -> Chvostek's (face twitching) ->
bronchospams -> prolonged QT

ICU BASICS & CARDIO
PRESSORS
Norepinephrine (Levophed)
Half life 2.4 min. Start 1 mcg /min and titrate q3min until map 65 max of 14 mcg/min.
Beyond 14 mcg requires Central Line max of (50mcg /min) = take BP q 15 min + Urine output (Oliguria = 20mL/hr)
a > b receptor profile
0.01 - 0.05 mcg / kg/ min (microgram)
beyond 0.05 dosing / kg/ min would cause deminished return with ischemic limbs
Impacted by the pH of the body.
first line
Vasopressin V1
0.03 - 0.04 units/min
not pH dependent and can wean off more levophed
mesenteric ischemia risk
Phenylephrine a agonist
reflex brady risk (do not use on brady person) also do not use in obstructive shock (like Pulm Embolism)
Epinephrine b>a
- increase heart output (good for brady)
Dopamine (SOAP II trial showed significant high rate of arrythmia) good for low Systemic vascular resistence with some alpha
<3 - renal
3- 10 = b
>10 = a
Dobutamine b agonist = good for normal svr / fast titration
Milrinone phosphodiesterase inhibitor for ionotrope = good for increased SVR as Milrinone will vasodilate.
renally cleared ESRD contraidndicated
3rd / 4th pressor patient
give steroid hail mary throw
- hydrocortisone 50mg q6h or 100mg q8h
>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>
Analgesia and Sedation
Propofol
pros: quick on / off (10 min)
cons: hypotension, propofol infusion syndrome [acidosis, rhabdo, bradycardia] check TG q 3 days if >400, discontinue /move to next
green urine seen
5- 50 mcg /kg/min
can go up to 100 mcg /kg/min but i would be worried after crossing 60mcg/kg/min mark
Precedex (Dexmodetomidine)
- bradycardia risk
- good for agitation / ICU delirium
- good for spontaneous breathing trial as this drug has little effx on respiratory depression
- weaker than propofol
0,2 - 1.4 mcg/ kg/ hr
midazolam (Versed)
- ICU delirium *
- patient builds tolerance
- builds up in fat = takes long time for people to wash out
- neutral for BP
2- 20 mg/hr
* past 10 mg /hr = considered alot
Ketamine
- emergence reaction of K hole
- transient increase in HR + BP
8-25mg/hr ggt
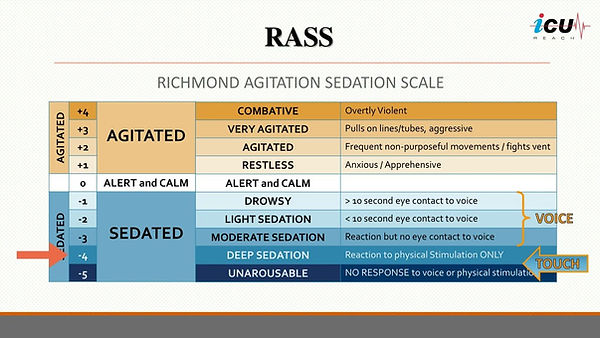
WEANING OFF OF SEDATION : RASS = Richmond Agitation -Sedation Scale
0 to -2 is a good place.
-3 perhaps for ventilator
Analgesia
Fentanyl
- first line neutral effect on BP
25 - 200 mcg/hr
Dilaudid
- hypotension
- opioid tolerant patient
- hepatic clearance
Morphine
- hypotension
- renal clearance
- decreases air hunger great for end of life care / comfort tx = antianxiolytic
Bowel regimen these patients and if they are not pooping for +5 days try methylnaltrexone (super expensive)
Paralytics
Acurasy's trial = paralysis has mortality benefit / Rose trial = no mortality benefit in first 48 hrs
We paralyze people so they dont fight the ventiliator thats why trial was even done and why we do paralytics
- MAKE SURE THE PATIENT IS SEDATED RASS OF -3 to -5
TRAIN of FOURS electrical signal down to peripheral nerves to check finger twitches / Bispectral index electrode on head works
- 4 twitch = 0- 75% receptors blocked
- 3 twitch = at least 75% receptors blocked
- 2 twitch = 80% R blocked
- 1 twitch = 90% R blocked
- 0 twitch = 100%
- ICU myopathy (muscle wasting) due to Paralysis
Cisatracurium (GGT) Nimbex
0.15 - 0.2 mg /kg /hr ggt
half life of 20 - 30 min
Rocuronium (Zemuron) - more of a push drug rather than ggt
0.6 mg/kg
Vecuronium (Nocruon)
AFIB & BEYOND
Medical student level
AFIB = foci around L Atrium near the pulm vein "irregularly irregular"
Causes : PIRATES
-Pulmonary Pneumonia, post op, PE
-Ischemia
-Rheumatic structural
-Anemia / alcohol
-Thyroids / toxins
-Electrolyte ; endocarditits
-Sepsis/surgery
Complications: stroke /TIA AFIB with RVR hemodynamic compromise and Tachycardia mediated HF (cardiomyopathy)
CHADVASC2 & HASBLED SCORE
INTERN LEVEL
AFIB location = left atria pumonary vein (no wonder why COPD and AFIB go together so well)
AFLUTTER location = R Atrium Cavotricuspid isthmus (Re-entrant loop)
Definitive treatment (not 100%) =Ablation or Maze procedure (cutting around Atrium = maze no electrical signal)
-risk of surgery = bleeding in the Esophagus due to cautery
Duration of AFIB
- paroxysomal AFIB = intermittent and less than 7 days
- persistent AFIB = more than 7 days
- Longstanding persistent = greater than 1 yr
- permanent AFIB = tried multiple therapies / ablations and still has em
Valvular / NonValvular AFIB
- Valvular = mechanical valve replacement or rheumatic mitral stenosis
tx = Warfarin
- Nonvalvular = DOAC
TREATMENT
AFFIRM trial = rate and rhythm control noninferior to one another
RACE TWO TRIAL compared mortality between HR < 80 vs HR <110. Approach of allowing 110 HR had better outcome
East AFNET4 trial states rhythm control : new afib patient with early rhythm control had better mortality, stroke, HF risk
however this is including fleconide dronedarone AND ablation vs betablocker traditionally = misleading
Goal HR < 110
Rate control agents to choose: (tend to cause brady / hypotensive)
Metoprolol #1
- 2.5 to 5 mg IV q5min x 3 if it doesnt work go to diltiazem
- good for people who has hyperthyroidism (blocking T4-T3 conversion)
- avoid in reactive airway disease
- adverse rxn of AV blocking, hypotensive, bradycardia
Diltiazem ggt #2
- 0.25 mg /kg (~ 20mg bolus) and then 0.35mg/kg bolus then to ggt keep it at 0.10 - 0.15 mg/kg/hr ....which is roughly 5 - 10 mg/hr
- check out IV to oral conversion on uptodate
- great at blocking AV block (better than metoprolol)
- blackbox warning = avoid with systolic HF
Digioxin
- 0.5 mg bolus then 0.25 mg q6h twice (1mg loading done) / 0.125 - 0.25 mg dosed daily
- good if hypotensive / HF
- bad because slow onset (2hr), digioxin measured q2wk, only pick up if poorly controlled despite metoprolol/diltiazem
Esmolol
500mcg/kg bolus then ggt look up on uptodate
- good for rapid titration
- bad because it provides ton of volume (overload)
Rhythm control agents to choose:
Amiodarone
- good if hypotensive
- also has rate control property
- chemical cardioversion good but make sure to = anticoagulate patient
DO NOT GIVE metoprolo, diltiazem, digioxin, esmolol, amiodarone if they have pre-excited afib
- pre-excited afib = wide QRS / WPW
you must use procainamide or electrical cardioversion instead
Hemodynamically unstable = cardioversion route
Summary:
Metoprolol good 1st line
Diltiazem is strong but avoid in HF / Verapamil uncommon.
Digioxin is good if HF and hypotensive
Esmolol if you not sure if they will be tolerating bb (ggt)
amiodarone use if hypotensive
Pre-excited give procainamide or electrical cardioversion
check electrolyte. abnormality will not allow meds to work
? Appropriate response to rate control : 20% reduction in HR, conversion to SR or HR less than 100 bpm
? AFIB with RVR developing HF: tachycardia mediated cardiomyopathy (takes weeks)
? Afib or Aflutter harder to rate control: Aflutter is harder consider earlier cadioversion or ablation
Chronic med in Afib/flutter
- BB in CAD / HFrEF
- CCB in COPD / Lung
- Digioxin added if above not adequate
- never combine bb ccb
Chronic meds rhythm control = all proarrythmic
- Amiodarone the big gun, most side effects and CYP450 inhibition. Avoid in Young pts (half life 1 month)
Need 10-14g loading dose
IV bolus and then GGt
400 mg BID 1 week then 100 - 200 mg daily
Baseline PFT, TFT, electrolyte q 3-6 month
- Dronedarone gentler version. fulminent hepatitis rare.
- fleconide and propafenone Class IC : cannot be used in structural heart dz (no MI , no valvular , dilated atria )
Pill in the pocket strategy = rate control pill pt takes this once they feel it coming on
- Dofetilide and Sotalol Class III - prolonged QTC; usually for ppl who has failed other therapies
NEW ONSET AFIB
unstable = cardiovert
stable = rate control
DId it start <48 hours ? > 48 hours?
<48 hours = cardioversion without anticoag
>48 hours = TEE and then cardioversion after confirming no clot
>48 hours = RACE 7ACWAS (2019) delayed cardioversion isnt bad compared to 4 wks vs immidiate
RACE 7ACWAS (2019) - 69 % of patients will spontaneously convert (AC) so you could just anticoag 3 wk and then do it later.
RAPID INTUBATION SEQUENCE
(for 100kg)
- Rocuronisum = paralytics
- Ketamine 1.5-2 mg/kg IBW.
- Etomidate 0.3-0.4 mg/kg TBW.
- Fentanyl 2-10 mcg/kg TBW.
- Midazolam 0.1-0.3 mg/kg TBW.
- Propofol 1-2.5 mg/kg IBW + (0.4 x TBW) (others simply use 1.5 mg/kg x TBW as the general guide)
- Thiopental 3-5 mg/kg TBW.
- Propofol = 0- 50 mcg / kg /min
https://litfl.com/rapid-sequence-intubation-rsi/
Day Shift
Discharge: med rec + discharge information (for patients) + summary (fellow doctors)
Discharge Med reconciliation can occur on the discharge tab on epic.
- You can order lab work (BMP) you can order referral
- Discharge information (briefly what happened tx and what to do appointment and meds)
- Discharge information (when to call for help)
- Print ahs section - point of view from patient's perspective
- Order: Discharge + Discontinue IV
Discharge Summary
1. Do it after orders and reconciliations
2. Main problem and treatment and follow up
3. To do list for PCP (BMP / Card follow up)
4. DC diagnosis & chronic / side problems
5. Procedures performed etc...
6. Per 9/16 H&P and copy and paste for HPI. Or brief summary in your own words.
7. Last progress note for hospital course A/P to copy paste.
SNF will require their own note* additionally.
PROGRESS / ROUNDING CHECKLIST (WORKING LIST)
Patient Name and (5 pertinent PMHX):
Room#
Problem List to direct physical exam and homeostasis:
Consults/Procedure coming up:
Daily Lab ***TRENDS
Lines:
Foley:
Vent/O2:
Diet & Ins Outs
GI PPx:
Bowel Regimen: Miralax 17g qAM / Senna 17.2g qHS &
IVF:
DVT/VTE PPx:
Antibiotics:
Cultures:
Isolation:
Code:
Med/recon:
Disposition:
LONGTERM GAME PLAN:

•